Introduction
Replacing a single Registered Nurse costs $61,110 on average, and with a national RN vacancy rate of 9.6%, healthcare organizations face a relentless cycle of expensive hiring. These vacancies push hospitals toward travel nurses who cost $79,090 more annually than permanent staff — bringing the average hospital's contract labor bill to $7.6 million per year.
Those costs aren't inevitable. They tend to grow when organizations default to agency staff, rely on manual screening, and let slow processes run without oversight. This article examines three dimensions of cost reduction: the decisions you make upfront, how you manage active hiring, and what drives those costs at the system level.
Key Takeaways
- Healthcare hiring costs accumulate through turnover cycles, agency markups, and extended vacancies, not as isolated one-time expenses
- Biggest drivers: 16.4% RN turnover, agency reliance at $79K+ premiums, and manual screening consuming 33+ recruiter hours weekly
- Cut costs by shifting agency-first defaults to internal pipelines, tightening role requirements, and investing in high-ROI sourcing channels
- AI interview tools compress time-to-fill from 83 days to weeks, freeing recruiters from manual screening
- Float pools, academic pipelines, and workforce analytics create structural savings that grow over time
How Healthcare Hiring Costs Build Up
Healthcare hiring costs rarely appear as a single budget line. They compound across stages: sourcing ads, recruiter screening hours, interview coordination, credentialing verification, and onboarding — each adding incremental cost that goes largely untracked until it becomes a crisis.
Key stages where costs quietly stack up:
- Sourcing and advertising — job board fees, sponsored listings, and recruiter time spent writing postings
- Screening and interviews — hours spent reviewing applications, scheduling, and conducting initial assessments
- Credentialing verification — licensing checks, background screenings, and compliance documentation
- Onboarding — orientation, training time, and the productivity lag before new hires contribute fully
The build-up is cyclical and self-reinforcing. Healthcare organizations lose between $3.9 million and $5.7 million annually due to RN turnover alone. With a 16.4% annual RN turnover rate and 22.3% first-year turnover, the hiring cycle restarts before previous hires reach full productivity — meaning organizations perpetually absorb the full cost sequence without ever breaking the loop.

What makes this cycle so costly is that most of it stays invisible. Fragmented tracking across recruiting, HR, and operations means no single team owns the full picture. When internal pipelines finally fail under vacancy pressure, organizations default to agency or travel staffing at premium rates — and that's when the accumulated inefficiency lands on the balance sheet all at once.
Key Cost Drivers in Healthcare Hiring
Healthcare hiring costs stem from a handful of recurring structural problems. Understanding each one is the first step toward fixing them.
Agency and Travel Staffing Premiums
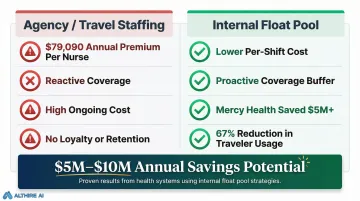
When internal hiring pipelines are slow or underdeveloped, healthcare organizations default to agency arrangements carrying significant markups. Travel nurses cost hospitals $79,090 more per year than permanent staff, with hourly rates of $93.81 versus $55.79 for permanent RNs. For every 20 travel nurses replaced with permanent staff, hospitals save approximately $1.58 million annually.
High Clinical Role Turnover
Bedside nursing, medical assistants, and allied health positions carry above-average attrition rates. Respiratory therapists face 15.2% annual turnover, while first-year RN turnover reaches 22.3%. Each departure triggers a full re-hire cycle — sourcing, screening, credentialing, and ramp-up — compounding hiring demand with every exit.
Manual and Unstructured Screening Processes
Unstructured phone screens, back-and-forth scheduling, and inconsistent evaluation criteria extend time-to-fill and consume disproportionate recruiter hours. RN positions take 83 days to fill — nearly double the 44-day general industry average. Recruiter time is a real cost that rarely gets attributed to cost-per-hire calculations.
Credentialing and Compliance Overhead
Healthcare uniquely requires license verification, background checks, and role-specific credential validation before hires can work. When handled manually and sequentially rather than in parallel, these steps add 60 to 180 days to the hiring timeline. For physician hires specifically, the administrative burden breaks down like this:
- Time investment: 20–40 hours per hire in administrative processing
- Direct labor cost: $400–$1,200 per physician credentialing cycle
- Root cause: Sequential (rather than parallel) verification workflows
Extended Time-to-Fill Driving Downstream Costs
Every unfilled clinical role generates real downstream cost. Existing staff absorb overtime. Patient capacity tightens. Agency coverage fills the gap at a premium. The NSI National Health Care Retention Report estimates the cost of a single RN turnover at $56,300 on average — making time-to-fill one of the highest-leverage variables in healthcare hiring cost control.
Cost-Reduction Strategies for Healthcare Hiring
No single strategy reduces healthcare hiring costs across all organizations. Effective cost reduction depends on diagnosing whether costs are driven by upfront decisions, active management gaps, or structural factors surrounding the hiring process.
The strategies below are grouped by where they intervene — in the decisions made before hiring begins, in how the process is managed once it starts, and in the broader systems that shape hiring demand.
Strategies That Reduce Costs by Changing Hiring Decisions
Make internal staffing the default, not the fallback
Many healthcare organizations treat agency staffing as a first response rather than a last resort. Shifting to an internal-first policy with clearly defined escalation criteria — for example, "agency engagement begins only after 30 days open" — can meaningfully reduce premium spend without compromising fill rates.
Audit role requirements before posting
Inflated job requirements shrink the qualified candidate pool unnecessarily. Asking for experience levels or credentials beyond what the role actually demands extends time-to-fill and increases sourcing costs. Review minimum qualifications against real role complexity to widen your candidate pipeline.
Concentrate sourcing spend where conversion data points
Healthcare organizations often spread spend across general job boards when role-specific platforms produce lower-cost, faster-converting candidates. Track source-of-hire data to identify which channels deliver the best cost-per-qualified-applicant. Employee referral programs and nursing-specific boards typically outperform generic platforms.
Treat retention as a hiring cost strategy
The highest-leverage decision for cutting long-term hiring costs is reducing voluntary attrition. Every avoided departure eliminates a full hire-cycle cost. Evaluate exit interview data to identify actionable retention levers: scheduling flexibility, onboarding quality, and compensation benchmarking.
Strategies That Address How Hiring Is Managed
Automate early-stage screening to recover recruiter capacity
The phone screening and first-round interview stage is where recruiter hours accumulate fastest. Replacing these with AI-powered interview tools lets candidates complete structured, asynchronous interviews on their own schedule. AltHire AI, for instance, conducts 24/7 interviews with adaptive follow-up, objective scoring, and detailed candidate reports, reducing the 33+ recruiter hours per week typically consumed by manual screening.
Run credentialing in parallel, not in sequence
Credential checks, license lookups, and background screening are often started only after an offer is accepted. Shifting these steps to run concurrently with later interview stages removes days of sequential delay at minimal added cost.
Measure cost-per-hire by role, not just organizationally
Cost reduction without measurement is guesswork. Tracking cost-per-hire, source-of-hire efficiency, and offer-acceptance rates by role type reveals which departments or job families are cost outliers — and points to root causes that aggregate numbers hide.
Standardize panel structures to cut scheduling delays
Coordinating multiple clinical managers for interview panels is one of the most underestimated causes of time-to-fill delays. Standardizing two-stage interview structures and using ATS-integrated scheduling tools removes the back-and-forth that routinely adds a week or more to the hiring timeline.
Structural Strategies: Reducing Hiring Demand Itself
Build internal float pools before the next vacancy hits
Organizations without internal float or per-diem capacity have no buffer against vacancies except expensive agency coverage. The savings potential is real: Mercy Health System cut agency spend by 50%, saving over $5 million by creating an internal gig workforce. A separate hospital expanded its float pool and reduced traveler nurse usage by 67%, with an estimated $10 million in savings.
Partner with training programs to build a pre-qualified pipeline
Partnering with nursing schools, allied health training programs, or medical assistant certification bodies creates a lower-cost, pre-qualified candidate supply. Jefferson Health's Capstone Program achieved hire rates of 50–52% of participating students, with 92% retention beyond the first year. These relationships take time to build but deliver lasting cost savings that grow as the pipeline matures.
Use predictive data to open roles before vacancies become urgent
Reactive hiring is always more expensive than proactive hiring. Organizations that use historical turnover patterns to open roles 60–90 days before anticipated vacancies can source at full quality rather than under pressure. Machine learning models can predict turnover within a 3–12 month window with 75–90% accuracy — enough lead time to build a pipeline before the seat goes empty.
Conclusion
Effective healthcare hiring cost reduction starts with understanding where costs actually originate—upfront decision gaps, management inefficiencies, or over-reliance on agencies—then addressing each layer deliberately rather than making across-the-board budget cuts.
The organizations that sustain savings over time focus on four things:
- Tracking cost-per-hire data consistently to spot where spend concentrates
- Automating low-value screening tasks to free recruiter capacity
- Reducing turnover by improving hiring fit from the start
- Building proactive talent pipelines that reduce reactive, high-cost sourcing
These aren't one-time fixes. Each compounds on the others, and the gap between organizations that act on them and those that don't widens with every hiring cycle.
Frequently Asked Questions
How to reduce hiring costs?
Reducing hiring costs starts with identifying your highest-spend drivers. The most common levers are:
- Reducing agency reliance
- Automating screening to cut recruiter hours
- Improving retention to lower re-hire frequency
- Tracking cost-per-hire data to pinpoint where spend is highest
What is the average cost-per-hire in healthcare?
The average cost of turnover for a staff RN is $61,110, with a range of $49,500 to $72,700. This figure rises significantly when agency placements or extended vacancies are factored in, as travel nurses cost $79,090 more per year than permanent staff.
How does high turnover increase healthcare hiring costs?
Each voluntary departure triggers a full re-hire cycle—sourcing, screening, credentialing, and onboarding. With RN turnover at 16.4% annually and first-year turnover at 22.3%, reducing attrition by even a small percentage has an outsized impact on total annual hiring spend.
What role does AI play in reducing healthcare recruitment costs?
AI-powered interview tools automate the most time-intensive screening stages, allow 24/7 candidate assessment, and produce objective scoring that reduces the recruiter hours and scheduling delays that drive up per-hire costs. Platforms like AltHire AI save 33+ recruiter hours per week through automated screening.
How can healthcare organizations reduce their reliance on staffing agencies?
Build internal alternatives first: float pools, per-diem programs, and academic pipelines. Then set clear policy thresholds defining when agency use is authorized, rather than treating it as the default response. Organizations that implemented float pools saved $5–$10 million annually.
What is the fastest way to reduce time-to-fill in healthcare hiring?
Running credentialing steps simultaneously, automating first-round screening with AI interview tools, and standardizing interview panel structures are the three fastest actions for compressing time-to-fill without sacrificing candidate quality. These changes can reduce the average 83-day RN time-to-fill by weeks.